📊 BMI & Procedure Eligibility Calculator
Enter your height and weight to see your BMI, what it means clinically, and whether you may meet the general criteria for bariatric surgery. This is a starting point for your conversation with a surgeon — not a determination of eligibility.
Actual surgical eligibility requires a full medical evaluation including health history, comorbidities, and surgeon assessment. This calculator is for general educational purposes only. Always consult a qualified bariatric surgeon.
Enter Your Measurements
What You Are Actually Choosing
When patients research bariatric procedures they typically find simplified comparisons — sleeve loses X%, bypass loses Y%, sleeve is easier recovery, bypass is better for diabetes. These comparisons are not wrong. They are incomplete. And incomplete information about a permanent, irreversible decision is dangerous.
The procedure that is right for you depends on factors that are specific to you — your anatomy, your health conditions, your reflux history, your diabetes status, your medication needs, your lifestyle, your risk tolerance, and your surgeon's clinical judgment about your individual situation. This page gives you the full clinical picture so that when you have that conversation with your surgeon, you are having it with real information.
The Most Important Thing On This Page
Long-term success depends more on behavior and support than on which procedure was performed. The best procedure for you is the one that matches your specific health profile, anatomy, and risk tolerance — chosen in genuine collaboration with a surgeon who explains the reasoning clearly. Not the one a support group recommended, not the one your friend had, and not the one with the fastest early weight loss.
🔪 Sleeve Gastrectomy (VSG)
The gastric sleeve is currently the most commonly performed bariatric procedure in the United States. Approximately 70 to 80 percent of the stomach is surgically removed, creating a narrow tube — or sleeve — roughly the size and shape of a banana. The remaining stomach functions normally; the digestive pathway is unchanged.
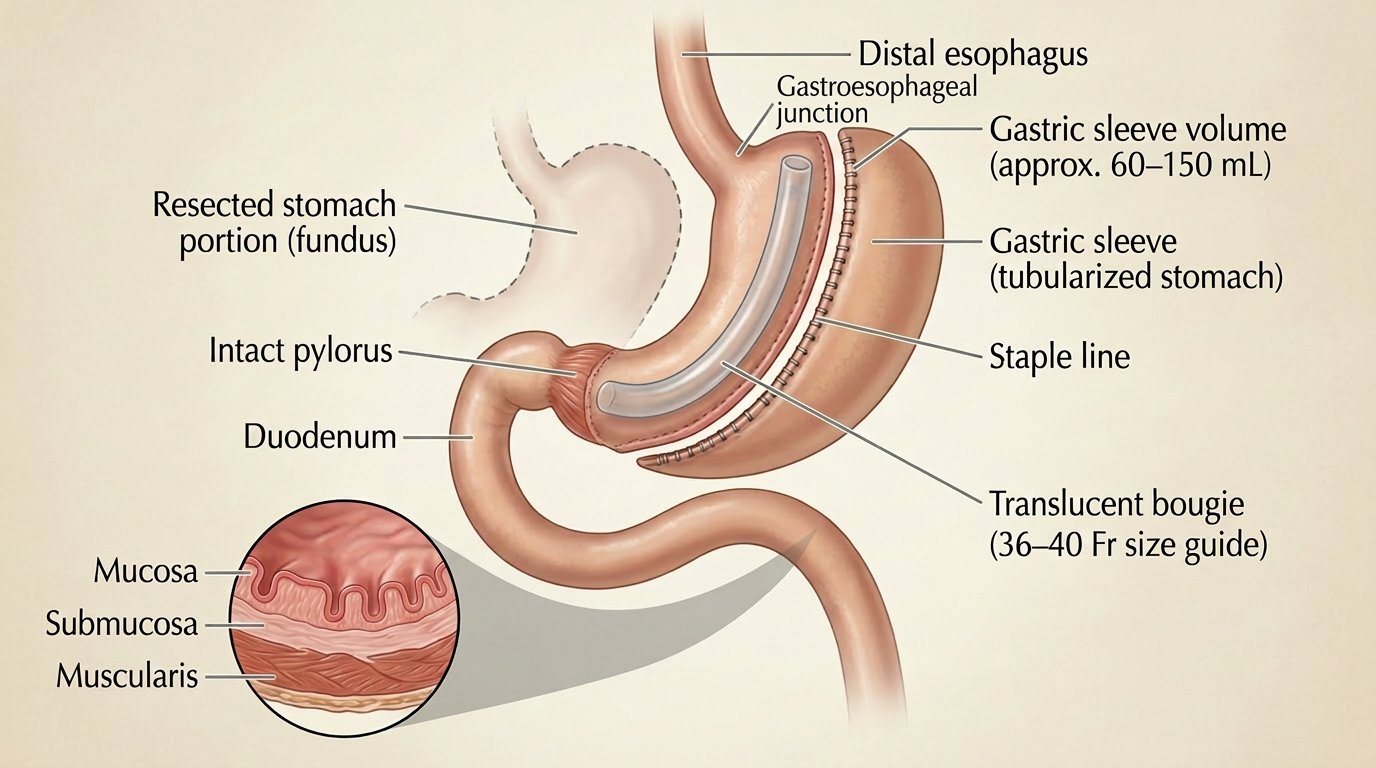
How It Works
- Restriction only — significantly reduces stomach capacity; no intestinal bypass or rerouting
- Ghrelin reduction — the removed portion of the stomach produces the majority of ghrelin, the primary hunger hormone. Removing it reduces hunger significantly — particularly in the first one to two years post surgery.
- Irreversible — the removed stomach tissue is gone. This cannot be reversed.
Typical Outcomes
- Excess weight loss — approximately 60–70% at two years in most studies
- Strong early weight loss — rapid loss in months one through twelve is typical
- Fewer nutrient deficiencies than bypass — the digestive pathway is unchanged, so absorption is less affected. Supplementation is still required for life.
- Comorbidity improvement — significant improvement in type 2 diabetes, hypertension, sleep apnea, and joint disease. Diabetes remission rates are lower than bypass.
- Technically simpler surgery — shorter operating time and lower early complication rate compared to bypass in most studies
Considerations and Limitations
- Reflux and GERD — this is the most important sleeve-specific concern. Sleeve gastrectomy can worsen acid reflux in a significant subset of patients. Patients with pre-existing GERD, Barrett's esophagus, or hiatal hernia should discuss this risk specifically and thoroughly with their surgeon. Some patients who have a sleeve eventually require conversion to bypass due to uncontrollable reflux.
- Slightly higher long-term regain rates — some studies show higher regain rates at five and ten years compared to bypass, though results vary significantly across study populations
- Sleeve dilation — the sleeve can stretch over time, increasing capacity and contributing to regain. This is a long-term anatomical factor, not a surgical failure or patient failure.
- No reversal option — unlike the band, this cannot be undone
✓ Sleeve may be a strong choice if: You have minimal or no GERD. You prefer a procedure that preserves the normal digestive pathway. You have lower malabsorption risk tolerance. Your surgeon assesses your anatomy and health profile as a good sleeve candidate.
⚠️ Discuss carefully if you have: Significant pre-existing GERD or acid reflux. Barrett's esophagus. A hiatal hernia. History of esophagitis. These are not automatic disqualifiers — but they significantly change the sleeve risk-benefit analysis and require specific surgical discussion.
🔄 Gastric Bypass (Roux-en-Y)
Roux-en-Y gastric bypass is the most studied bariatric procedure with the longest long-term outcome data. A small stomach pouch — roughly the size of an egg — is created from the upper stomach. The small intestine is then divided and rerouted, connecting the lower portion directly to the new pouch and bypassing the majority of the stomach and upper small intestine.
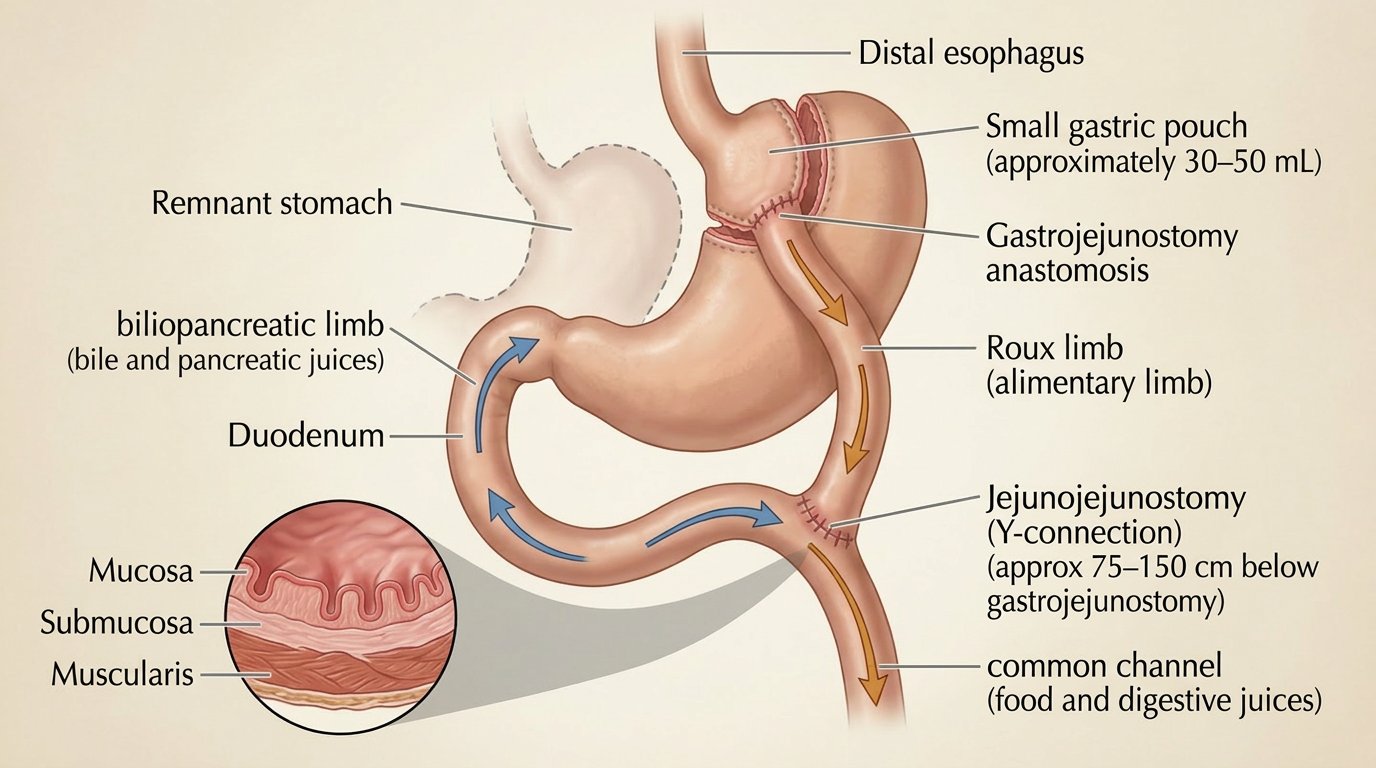
How It Works
- Restrictive and malabsorptive — reduced stomach capacity plus significantly reduced nutrient absorption from the bypassed intestinal segment
- Hormonal effects — bypassing the duodenum produces significant hormonal changes that drive rapid diabetes improvement, often independent of weight loss
- Acid reflux improvement — the anatomy of bypass physically reduces acid reflux for most patients. This is the opposite of the sleeve's effect on reflux.
Typical Outcomes
- Excess weight loss — approximately 70–80% at two years. Generally stronger long-term maintenance than sleeve in most long-term studies.
- Diabetes outcomes — gastric bypass produces some of the strongest documented type 2 diabetes remission rates of any intervention, including medication. Remission often occurs within days of surgery — before significant weight loss — due to hormonal changes.
- Reflux resolution — most patients with GERD experience significant improvement or resolution after bypass. It is the preferred procedure for patients with significant reflux disease.
- Strong long-term data — more long-term follow-up studies than any other bariatric procedure
Considerations and Limitations
- Higher nutritional deficiency risk — malabsorption affects iron, B12, calcium, vitamin D, and other nutrients more significantly than sleeve. Supplement compliance and lab monitoring are more consequential after bypass than after sleeve.
- Dumping syndrome — more common after bypass than sleeve due to the rapid gastric emptying created by the new anatomy. Early dumping (within 30 minutes of eating) and late dumping (1–3 hours after) are documented post-bypass risks. See the Nutrition page for full dumping syndrome protocol.
- Technically more complex surgery — longer operating time, higher early complication potential compared to sleeve at most centers
- Alcohol absorption change — the absorption change described in the Special Topics section is most pronounced after gastric bypass
- Medication absorption changes — the bypassed intestinal segment is where many medications absorb. Extended-release formulations are particularly affected. See the Special Topics page.
- Difficult to reverse — technically reversible in rare circumstances, but revision surgery carries significantly higher risk than primary surgery and is not undertaken lightly
✓ Bypass may be a strong choice if: You have significant GERD, acid reflux, or Barrett's esophagus. You have type 2 diabetes with a goal of remission. Your BMI is higher and you are a candidate for the stronger weight loss outcomes. You can commit to the more rigorous lifelong supplement and monitoring protocol.
🔬 Duodenal Switch (BPD/DS) and SADI-S
The duodenal switch combines a sleeve gastrectomy with a significantly longer intestinal bypass than gastric bypass. It is the most aggressive bariatric procedure in common practice and produces the greatest weight loss and metabolic effects — along with the highest nutritional risk and the most demanding lifelong management requirements.
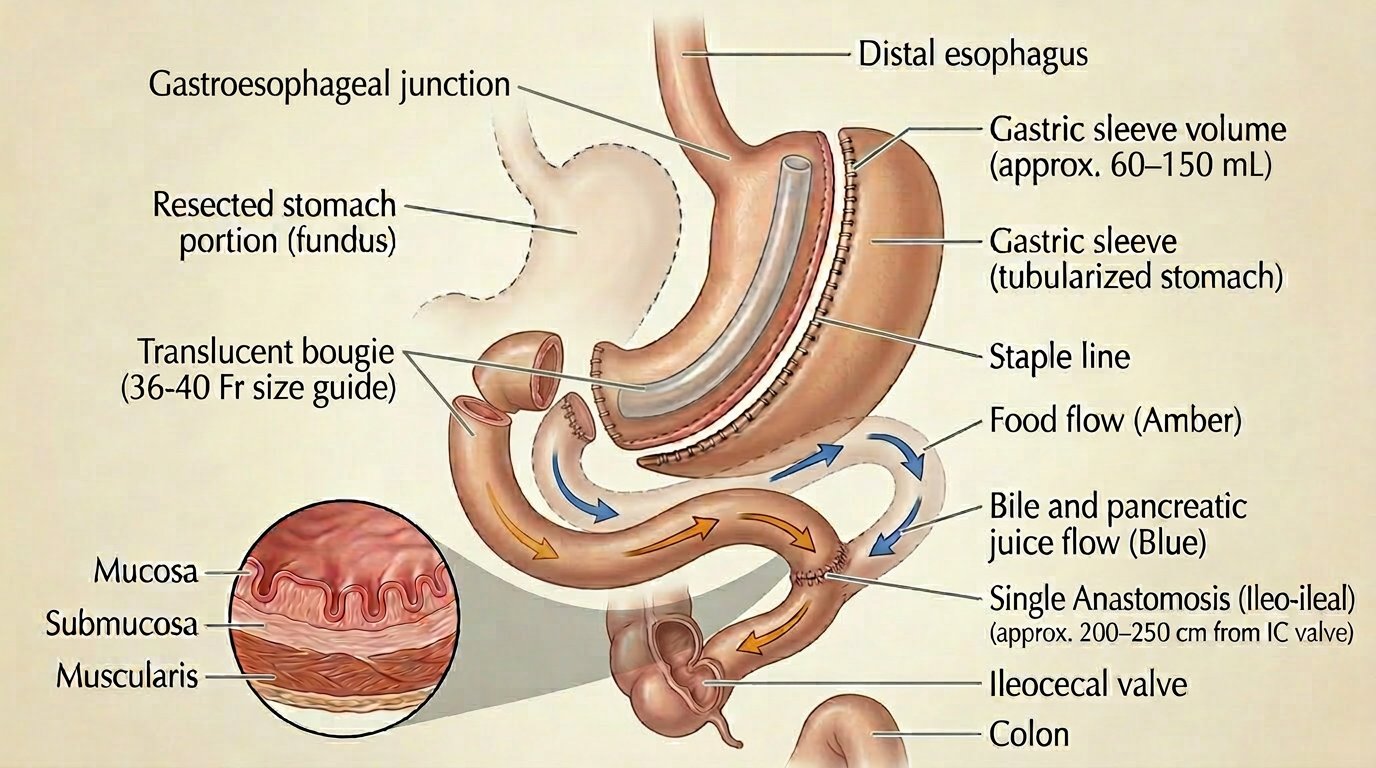
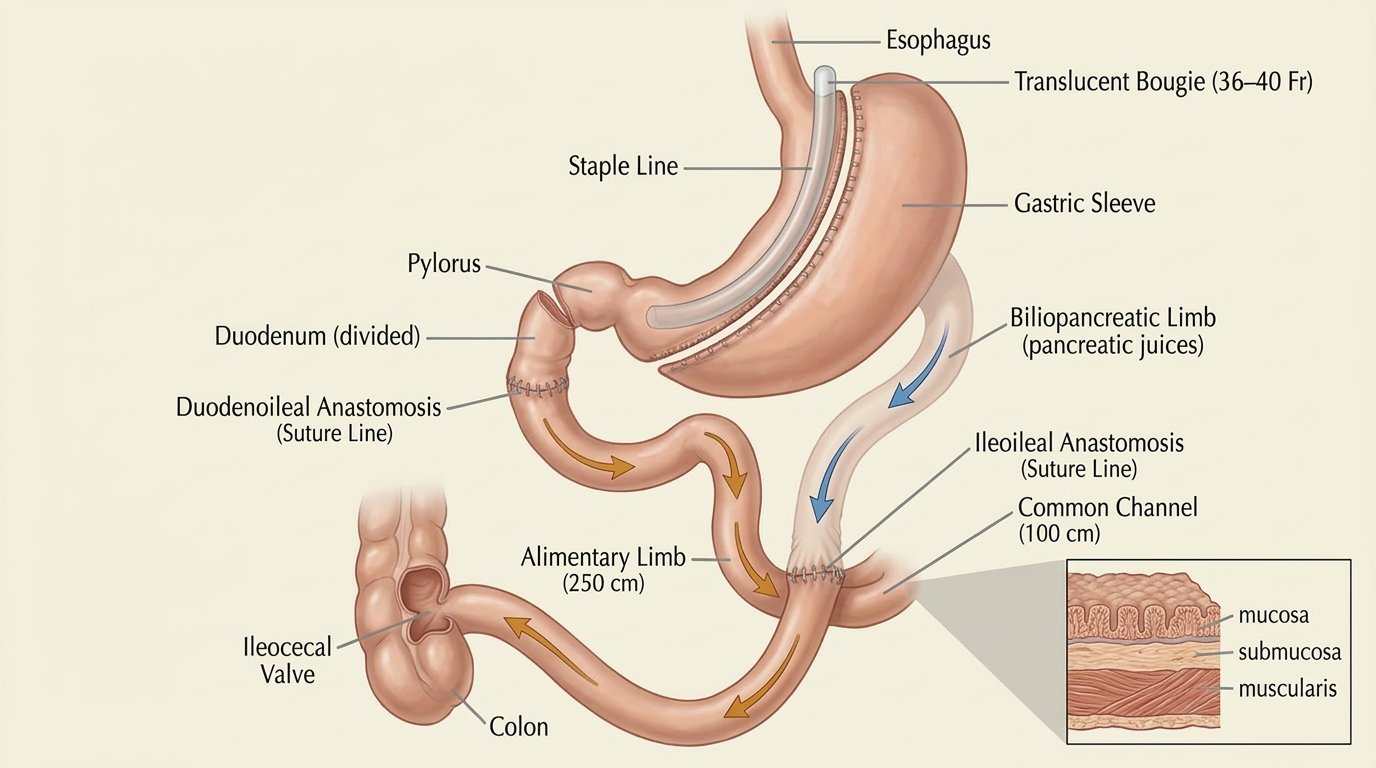
How It Works
- Sleeve component — 70–80% of the stomach is removed, identical to a standard sleeve
- Intestinal bypass — a much longer segment of small intestine is bypassed than in gastric bypass, dramatically reducing absorption of fat, calories, and fat-soluble nutrients
- SADI-S (Single Anastomosis Duodeno-Ileal Bypass with Sleeve) — a simplified version with one surgical connection instead of two, similar outcomes, increasingly preferred at centers offering DS
Typical Outcomes
- Greatest total weight loss of any commonly performed bariatric procedure — typically 70–80% excess weight loss or more
- Strongest metabolic effects — highest type 2 diabetes remission rates, significant improvement in metabolic syndrome
- Sustained long-term loss — the malabsorptive component continues contributing to weight management long term
Considerations and Limitations
- Highest nutritional deficiency risk of any procedure — fat-soluble vitamins (A, D, E, K), protein, iron, calcium, zinc, and copper are all significantly affected. Deficiencies that are manageable after sleeve or bypass can be severe after DS if supplements are not taken consistently.
- Most demanding lifelong monitoring — labs more frequently, supplement protocol more complex, dietary protein requirements higher
- GI side effects — loose stools, oily stools, and increased gas are common due to the degree of fat malabsorption. These can be significant quality-of-life factors.
- Not offered at all centers — requires a highly experienced surgical team. Verify your program's DS volume specifically before proceeding.
- Reserved for specific patients — most commonly recommended for patients with very high BMI (50+) or severe metabolic disease where the additional weight loss and metabolic impact justify the higher risk and management burden
📎 Adjustable Gastric Band
The adjustable gastric band was once widely performed and is now largely abandoned at most quality bariatric programs. It is included here because patients with existing bands still encounter care questions — and because understanding why it fell out of favor is clinically informative.
- An adjustable silicone band is placed around the upper stomach, creating a small pouch with an adjustable outlet
- No stomach removal, no intestinal bypass — fully reversible
- Weakest long-term weight loss outcomes of any bariatric procedure in the published literature
- High long-term revision and removal rates — band slippage, erosion, port complications, and inadequate weight loss drive very high reoperation rates over time
- Most quality MBSAQIP-accredited programs no longer offer the band as a primary procedure
- Patients who currently have a band and are experiencing inadequate outcomes or complications should discuss revision options with a bariatric surgeon experienced in band-to-sleeve or band-to-bypass conversion
How The Decision Gets Made — Individual Factors
No procedure is universally best. The right procedure is the one that matches your specific clinical profile, anatomy, and circumstances. Here is how surgeons and multidisciplinary teams approach the decision:
Factors That Influence Procedure Selection
- BMI and starting weight — higher BMI often favors procedures with greater weight loss potential (bypass, DS)
- Reflux and GERD history — significant GERD strongly favors bypass over sleeve. Barrett's esophagus is often a contraindication to sleeve.
- Diabetes status and severity — significant type 2 diabetes, especially insulin-dependent, often favors bypass for its superior diabetes remission outcomes
- Medication needs — patients on many medications where absorption changes could be clinically significant may favor sleeve
- Prior abdominal surgery — extensive prior surgical history affects which procedure is technically feasible
- Risk tolerance and lifestyle — the DS's outcomes come with the highest management demands; patient lifestyle and adherence capacity must match
- Supplement adherence history — patients with documented difficulty maintaining consistent supplement adherence may not be ideal bypass or DS candidates
- Surgeon recommendation based on individual anatomy — intraoperative findings occasionally change the planned procedure; discuss this possibility in advance
✓ The question to ask your surgeon: "Why are you recommending this specific procedure for my specific situation — and what is the clinical reasoning?" A complete answer addresses your health conditions, your anatomy, and the tradeoffs specifically. A vague answer or one that does not reference your individual factors is a reason to ask the question again, or to seek a second opinion.